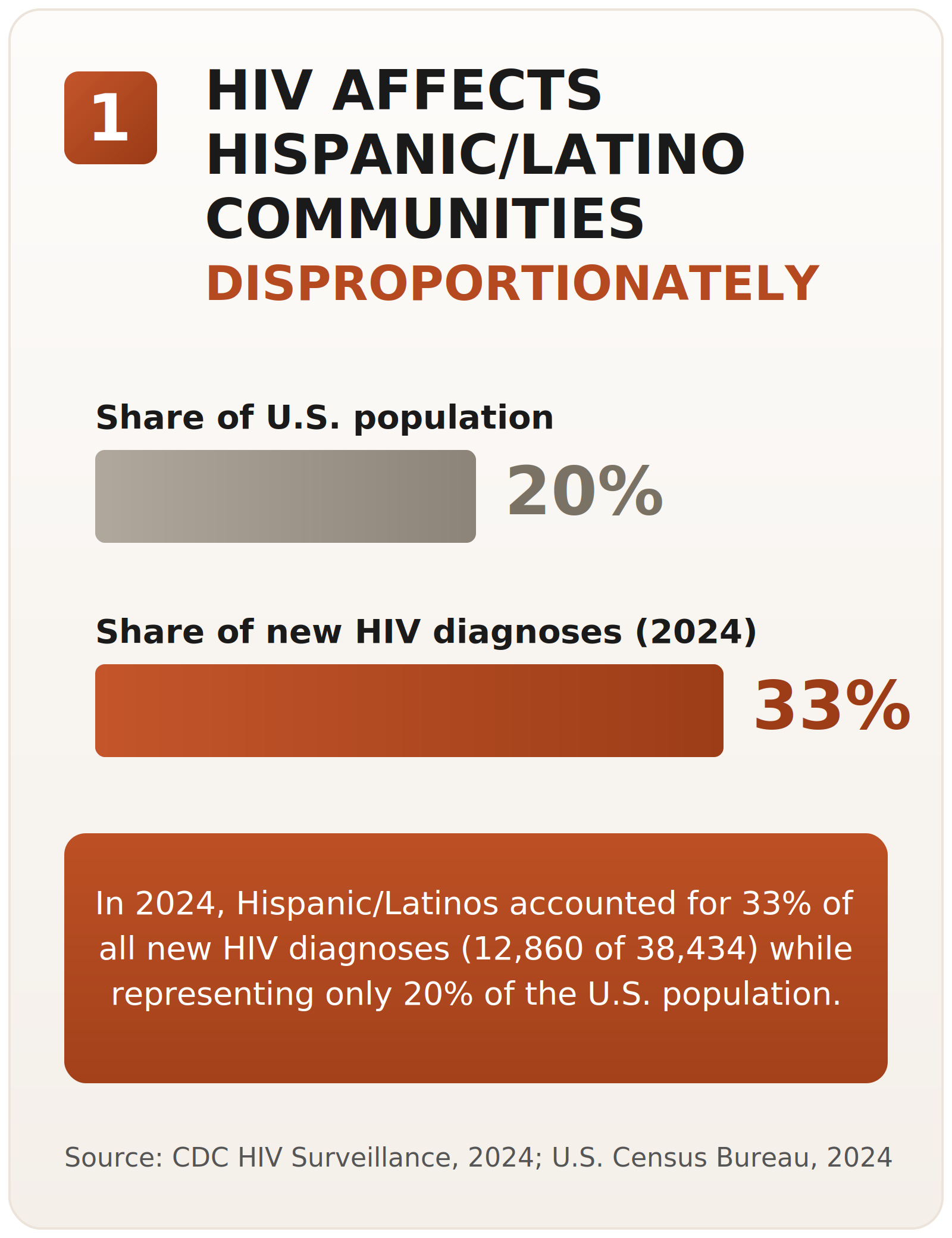
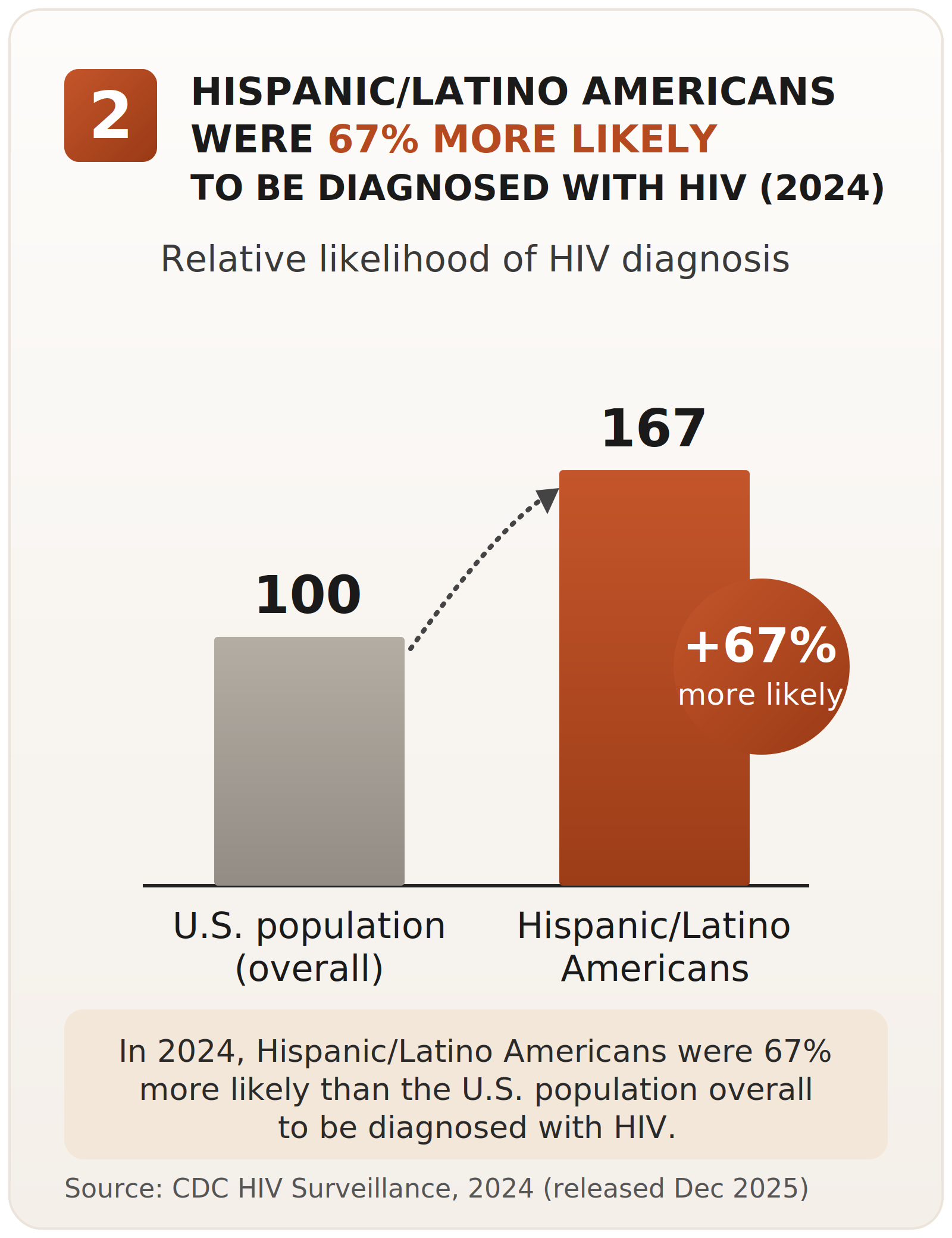
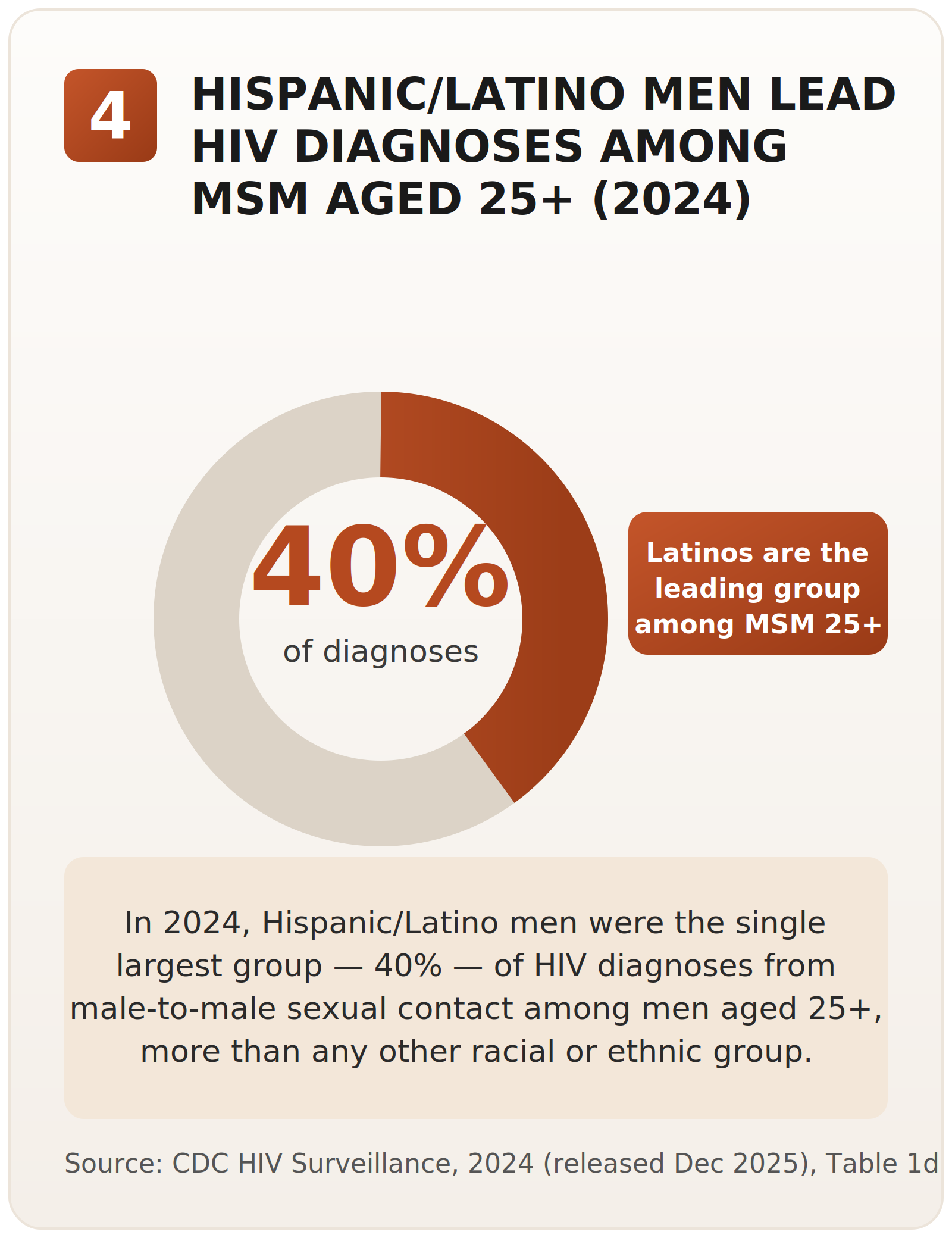
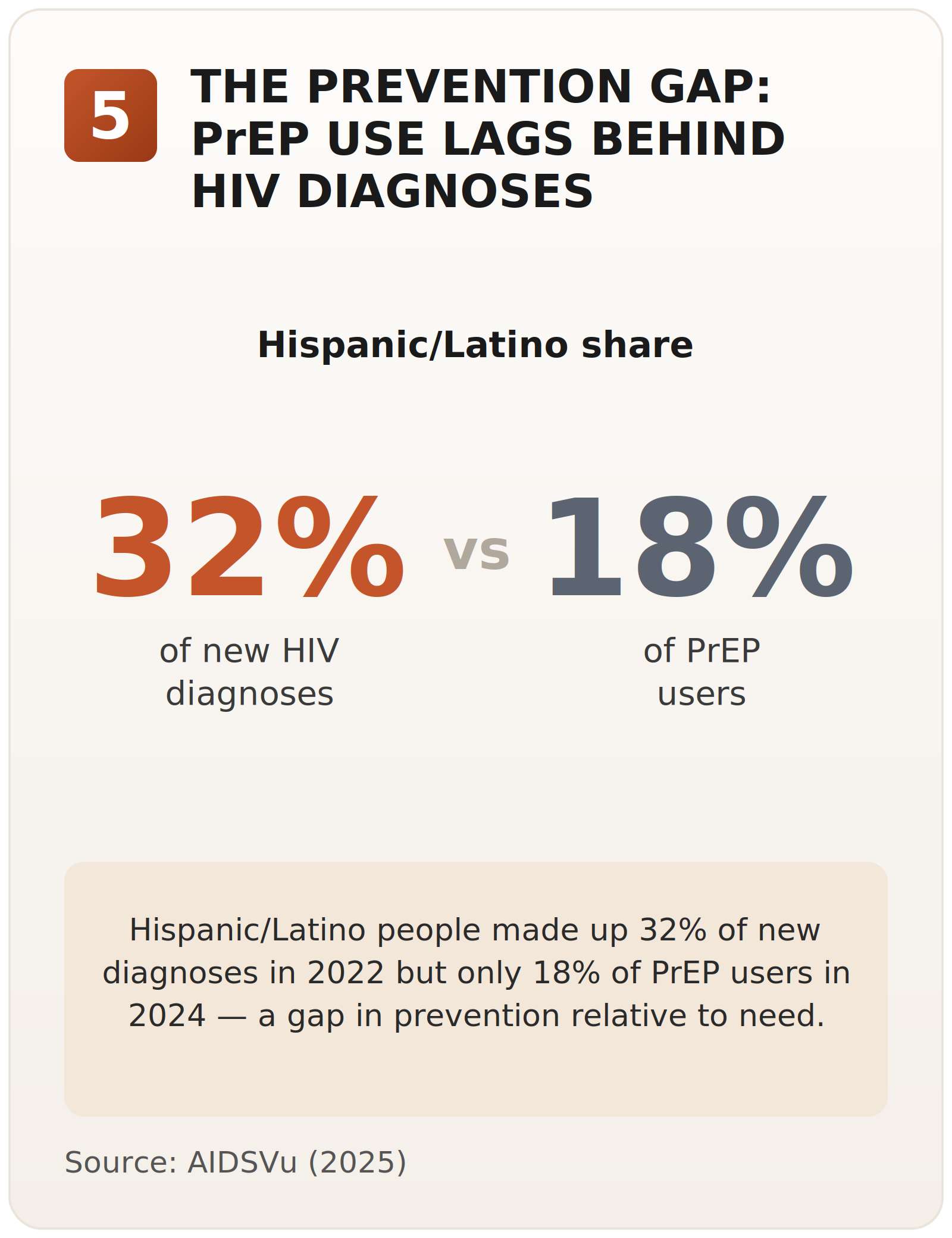
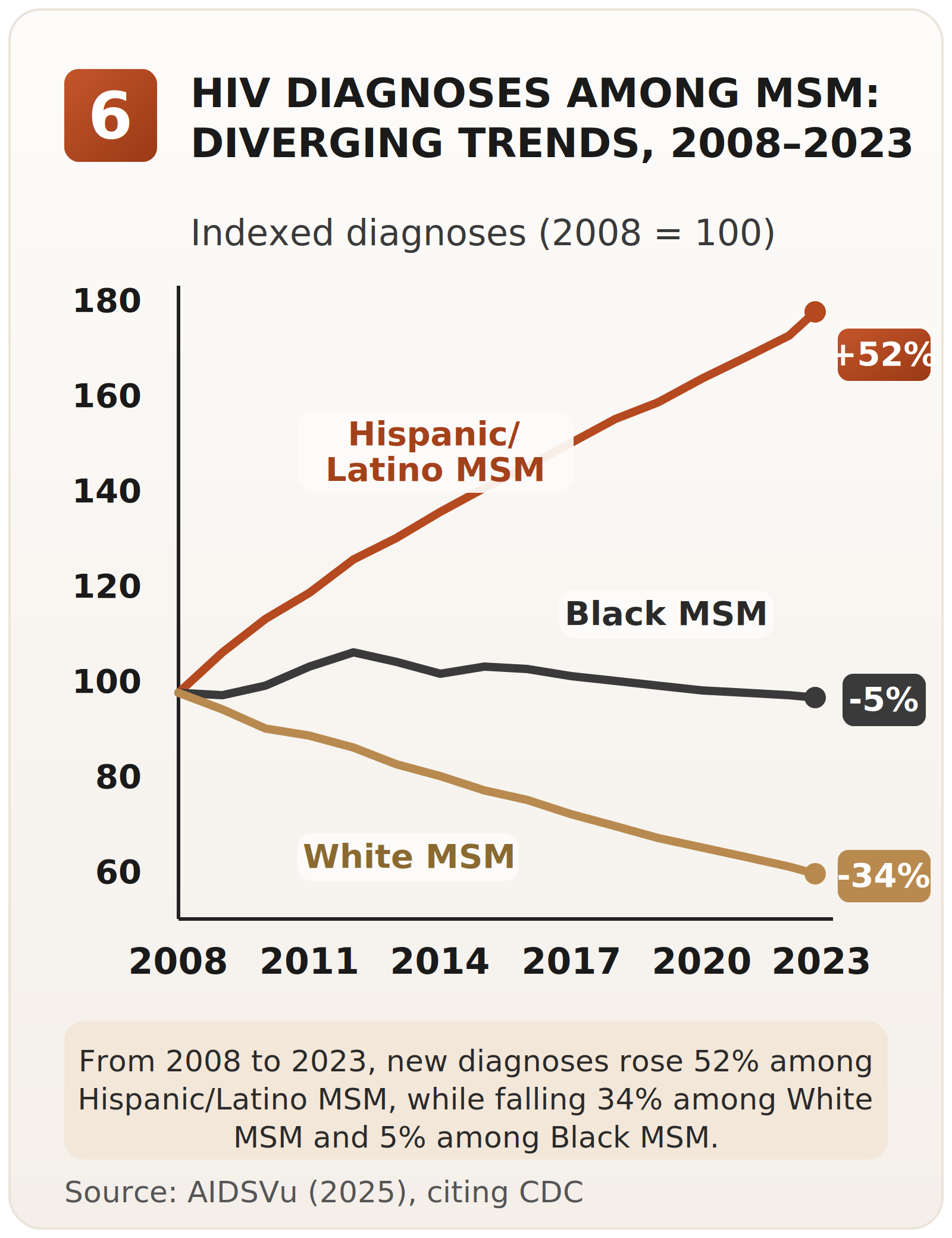
Latino/a/x communities in the United States have been disproportionately affected by HIV for decades.1 Newly released CDC surveillance data continue to show Hispanic/Latino communities carrying a disproportionate burden. In 2024, Hispanic/Latino people accounted for approximately one-third (34%) of new HIV diagnoses nationally, despite representing only 19% of the U.S. population. Among males aged 25 or older with HIV attributed to male-to-male sexual contact, Hispanic/Latino males accounted for 40% of HIV diagnoses.2 That is the starting point — even before the policy and funding shifts of 2025.Las comunidades Latinas/os/x en los Estados Unidos han sido afectadas de manera desproporcionada por el VIH durante décadas.1 Los datos de vigilancia recientemente publicados por los CDC siguen mostrando que las comunidades Hispanas/Latinas cargan con una proporción desmedida del VIH. En 2024, las personas Hispanas/Latinas representaron aproximadamente un tercio (34%) de los nuevos diagnósticos de VIH a nivel nacional, a pesar de constituir solo el 19% de la población de los EE. UU. Entre los hombres mayores de 24 años con VIH atribuido a contacto sexual entre hombres, los hombres Hispanos/Latinos representaron el 40% de los diagnósticos de VIH.2 Ese es el punto de partida — incluso antes de los cambios de políticas y financiamiento de 2025.
"Latinos have not been a priority. Infection rates amongst other groups and ethnicities are going down. Latinos are the only group that's going up.""Los Latinos no han sido una prioridad. Las tasas de infección en otros grupos y etnias están bajando. Los Latinos somos el único grupo que va en aumento."
Leader at a Community-Based Organization (PT01)Líder de una organización comunitaria (PT01)
What is happening now is not just more of the same.Lo que está ocurriendo ahora no es simplemente más de lo mismo. The strains described in this section were the ones that emerged most consistently across interviews and thematic analysis. They are by no means the only forces shaping Latino/a/x HIV care and community health in this moment, but they were the patterns participants returned to repeatedly across regions, professional roles, and organizational settings.Las tensiones descritas en esta sección fueron las que surgieron de manera más constante en las entrevistas y el análisis temático. De ninguna manera son las únicas fuerzas que moldean la atención del VIH y la salud comunitaria de las personas Latinas/os/x en este momento, pero fueron los patrones a los que los participantes regresaban una y otra vez, en distintas regiones, funciones profesionales y entornos organizacionales.
"I see it as if someone is plowing our future — economically and in terms of health. It's terrible for our communities.""Lo veo como si alguien estuviera arando nuestro futuro — económicamente y en términos de salud. Es terrible para nuestras comunidades."
Leader in Housing Services (PT18)Líder en servicios de vivienda (PT18)
Since early 2025, federal funding for HIV care and prevention has been cut in ways no organization can absorb without harm. The pattern is the same across regions: cuts came suddenly, with no phase-out or transition plan, and at a scale that forced immediate layoffs, service reductions, and program closures.Desde principios de 2025, el financiamiento federal para la atención y la prevención del VIH se ha recortado de maneras que ninguna organización puede absorber sin sufrir daños. El patrón es el mismo en todas las regiones: los recortes llegaron de manera repentina, sin un período de transición, y a una escala que obligó a despidos inmediatos, reducción de servicios y cierre de programas.3
"We are a $12 million organization, and on March 16th we lost a third of our funding. From one day to the next, about $4 million was cut. We had to reduce services and lay off staff across centers.""Somos una organización de 12 millones de dólares y el 16 de marzo perdimos un tercio de nuestro financiamiento. De un día para otro, se recortaron unos 4 millones de dólares. Tuvimos que reducir servicios y despedir personal en varios centros."
Leader at a Community-Based Organization (PT01)Líder de una organización comunitaria (PT01)
"A $5 million grant was completely eliminated. That funding supported sexual health services, community health workers, PrEP navigation, and testing for uninsured and underinsured patients.""Una subvención de 5 millones de dólares fue eliminada por completo. Ese financiamiento sostenía servicios de salud sexual, promotores de salud, navegación de PrEP y pruebas para pacientes sin seguro o con seguro insuficiente."
Leader at a Federally Qualified Health Center (PT11)Líder de un centro de salud federalmente calificado (PT11)
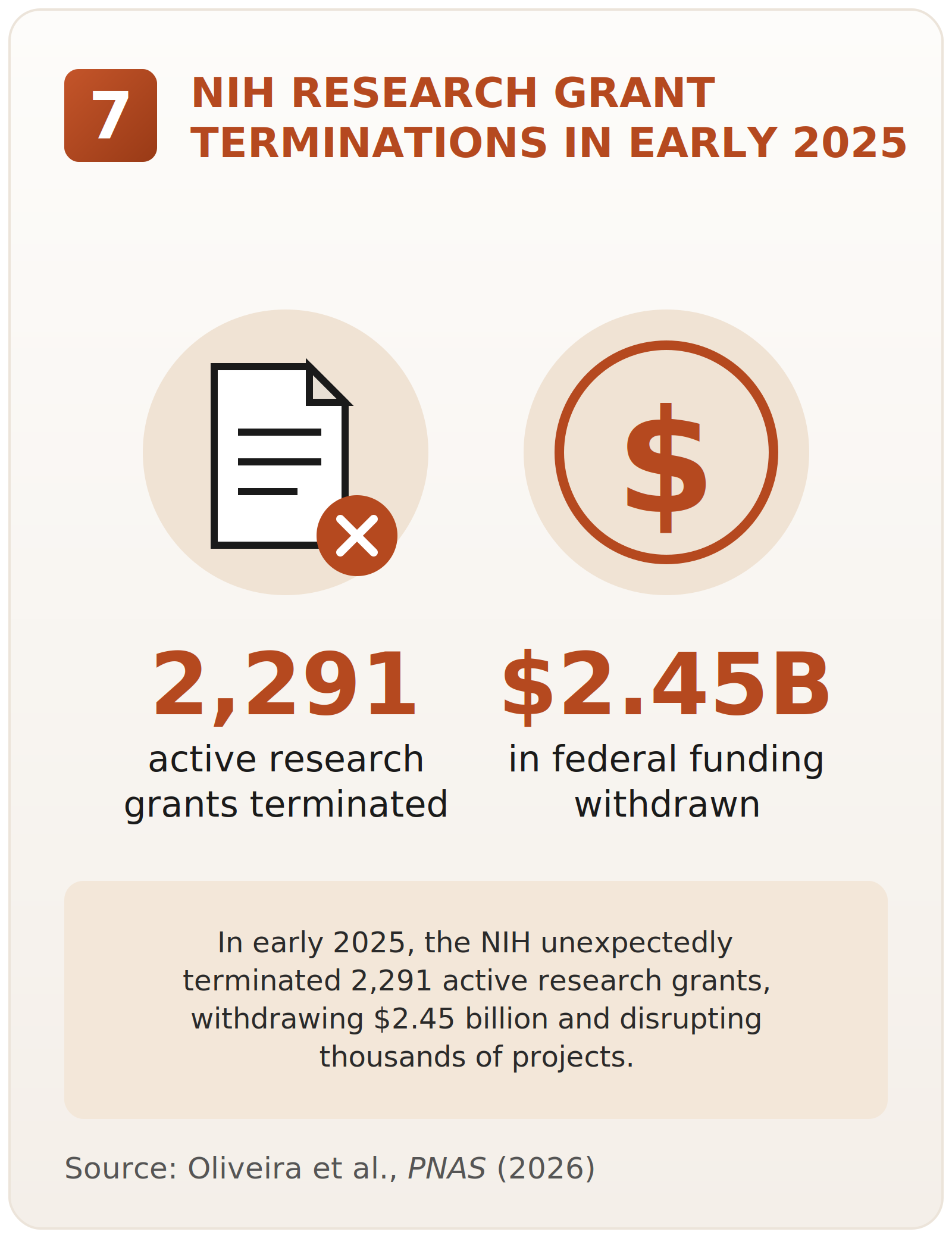
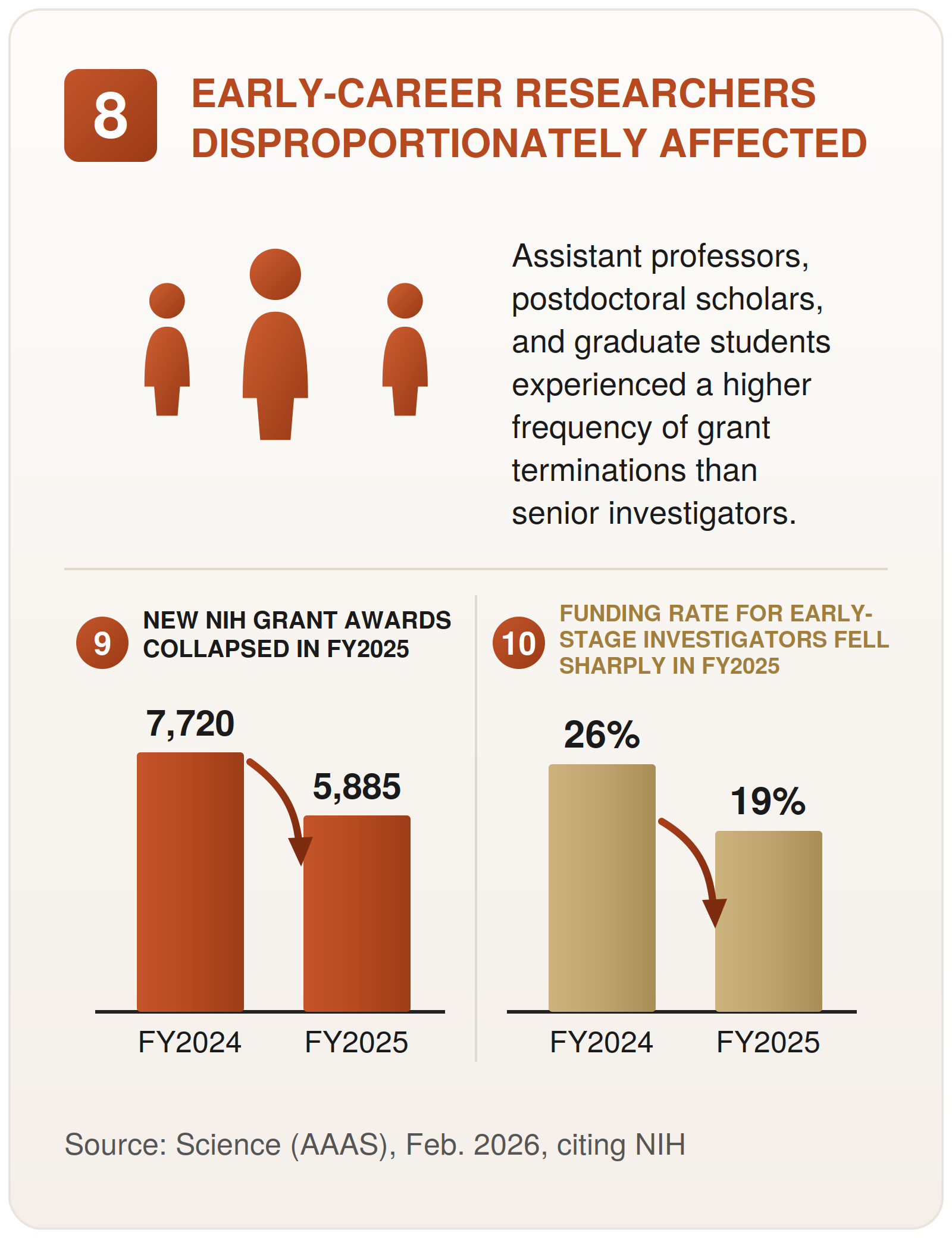
The cuts are hitting direct services and the research base behind HIV response and innovation.4,5Los recortes están golpeando los servicios directos y la base de investigación que sostiene la respuesta al VIH y la innovación.4,5
"At the beginning of 2025, I was affiliated with nine HIV-related research projects. Five of them were terminated.""A principios de 2025, yo estaba vinculado a nueve proyectos de investigación relacionados con el VIH. Cinco de ellos fueron cancelados."
HIV Researcher (PT04)Investigador de VIH (PT04)
These losses are not spread evenly. Programs serving Latino, LGBTQ, transgender, and other underserved communities have been hit the hardest.6,7 This is not a routine budget cut.8 It is a deliberate shift of public funding away from the communities and services most central to the HIV response.Estas pérdidas no se reparten de manera uniforme. Los programas que sirven a comunidades Latinas, LGBTQ, transgénero y otras comunidades desatendidas han sido los más golpeados.6,7 Esto no es un recorte presupuestario de rutina.8 Es un desvío deliberado del financiamiento público, alejándolo de las comunidades y los servicios más centrales para la respuesta al VIH.
Immigration enforcement is unfolding in Latino/a/x communities at a scale and intensity many participants described as unprecedented. It is no longer perceived as confined to specific individuals or formal legal processes, but as a visible and pervasive presence in public spaces, workplaces, near schools, and around the clinics and community organizations that provide care. As a result, many people are avoiding the very settings designed to support their health and wellbeing.9La aplicación de las leyes migratorias se está desplegando en las comunidades Latinas/os/x a una escala e intensidad que muchos participantes describieron como sin precedentes. Ya no se percibe como algo limitado a individuos específicos o a procesos legales formales, sino como una presencia visible y omnipresente en espacios públicos, lugares de trabajo, cerca de las escuelas y alrededor de las clínicas y organizaciones comunitarias que brindan atención. Como resultado, muchas personas están evitando justamente los entornos diseñados para apoyar su salud y su bienestar.9
"We used to have a 15–19% no-show rate. That increased to almost 50%. It's not just undocumented immigrants — permanent residents and U.S. citizens are afraid to go out because of indiscriminate raids.""Antes teníamos una tasa de ausentismo del 15 al 19%. Eso aumentó a casi el 50%. No son solo los inmigrantes indocumentados — los residentes permanentes y los ciudadanos estadounidenses tienen miedo de salir por las redadas indiscriminadas."
Leader at a Community-Based Organization (PT01)Líder de una organización comunitaria (PT01)
"Our families are being torn apart. Most Latino people feel there is a risk just going to the supermarket, speaking with an accent, or gathering in places where there are a lot of Latinos. There is a constant fear of being targeted.""Nuestras familias están siendo separadas. La mayoría de los Latinos siente que hay un riesgo con solo ir al supermercado, hablar con acento o reunirse en lugares donde hay muchos Latinos. Hay un miedo constante de ser blanco de una redada."
Leader at a National Nonprofit (PT03)Líder de una organización sin fines de lucro de alcance nacional (PT03)
"You can walk three or four blocks in the city and see the police or the National Guard. It feels like living under military occupation.""Puedes caminar tres o cuatro cuadras en la ciudad y ver a la policía o a la Guardia Nacional. Se siente como vivir bajo una ocupación militar."
HIV Researcher (PT16)Investigador de VIH (PT16)
Latinos are being swept up as a group, not assessed as individuals based on documentation or legal process. This is not an unintended side effect. It is how enforcement is built. And it is producing widespread fear that blocks access to care, services, and daily life.A los Latinos se los detiene en masa, como grupo, sin evaluarlos como individuos según su documentación o un proceso legal. Esto no es un efecto secundario no intencionado. Es la forma en que está diseñada la aplicación de la ley. Y está produciendo un miedo generalizado que bloquea el acceso a la atención, a los servicios y a la vida diaria.
The infrastructure that connects low-income Latino/a/x communities to ongoing care — Medicaid, state-run insurance for undocumented residents,10 sliding fee scales, and Affordable Care Act coverage — is being dismantled through several changes happening at once. Any of these alone would matter. Together, they are stripping coverage from hundreds of thousands of people across the country.11
"The governor and legislature decided to stop enrolling undocumented people in Medicaid starting January 1st. On top of that, people now have to pay co-pays. A $40 co-pay is a major obstacle when someone is living paycheck to paycheck.""El gobernador y la legislatura decidieron dejar de inscribir a las personas indocumentadas en Medicaid a partir del 1.° de enero. Además, ahora la gente tiene que pagar copagos. Un copago de 40 dólares es un obstáculo enorme cuando alguien vive de un cheque al otro."
Leader at a Community-Based Organization (PT01)Líder de una organización comunitaria (PT01)
"Medicaid has been significantly reduced here. Sliding fee scales have been pushed to their minimum. A lot of people will lose their health insurance or have to pay a huge co-pay just to see a doctor.""Medicaid se ha reducido mucho aquí. Las escalas de tarifas según ingresos se han llevado al mínimo. Mucha gente va a perder su seguro de salud o va a tener que pagar un copago enorme solo para ver a un médico."
Leader at a Federally Qualified Health Center (PT11)Líder de un centro de salud federalmente calificado (PT11)
The mechanisms vary by state — eligibility cutoffs, shorter re-enrollment cycles, new co-pays, reduced sliding scales, laws that exclude undocumented residents, and a chilling effect on Affordable Care Act enrollment.12 The direction is the same everywhere: fewer people covered, fewer paths to care, and no real replacement system stepping in.13 At the same time, the safety net that has historically caught people losing primary coverage is itself under threat: nearly 20 states have adopted cost-cutting changes to their AIDS Drug Assistance Programs (ADAP), which are funded through the federal Ryan White HIV/AIDS Program and pay for HIV medications and insurance premiums for low-income people with HIV.14Los mecanismos varían según el estado — límites de elegibilidad, ciclos de reinscripción más cortos, nuevos copagos, escalas de tarifas reducidas, leyes que excluyen a los residentes indocumentados y un efecto disuasorio sobre la inscripción en el Affordable Care Act.12 La dirección es la misma en todas partes: menos personas con cobertura, menos vías de acceso a la atención y ningún sistema de reemplazo real que tome el relevo.13 Al mismo tiempo, la red de protección que históricamente ha amortiguado a quienes pierden su cobertura principal está ella misma amenazada: cerca de 20 estados han adoptado cambios de reducción de costos en sus Programas de Asistencia para Medicamentos contra el SIDA (ADAP), que se financian a través del programa federal Ryan White HIV/AIDS y pagan los medicamentos contra el VIH y las primas de seguro de las personas de bajos ingresos con VIH.14
Federal directives are doing two things at once. They are banning the words used to name specific communities in grants, reports, websites, and clinical research,15 and they are restricting the services those same communities can receive.16 These are not separate actions. Together, they amount to a deliberate and systemic erasure of entire communities from the institutions, protections, services, and systems meant to recognize, support, and safeguard their wellbeing.
"They want to eliminate us as a population. They want to make believe that we don't exist. By beginning to do that, they can limit the resources and access to comprehensive services we've had access to.""Quieren eliminarnos como población. Quieren hacer creer que no existimos. Al empezar a hacer eso, pueden limitar los recursos y el acceso a los servicios integrales a los que hemos tenido acceso."
Leader at a National Nonprofit (PT03)Líder de una organización sin fines de lucro de alcance nacional (PT03)
"We cannot use 'Latino,' we cannot use 'LGBTQ,' we cannot use 'Latinx,' we cannot use 'underserved communities.' They're saying yes, you can continue to provide services, but you cannot use any of this language.""No podemos usar 'Latino,' no podemos usar 'LGBTQ,' no podemos usar 'Latinx,' no podemos usar 'comunidades desatendidas.' Nos dicen que sí, que podemos seguir prestando servicios, pero que no podemos usar nada de este lenguaje."
Leader at a Community-Based Organization (PT01)Líder de una organización comunitaria (PT01)
This erasure is not symbolic. It is operational. It is the mechanism by which access, services, and visibility are being pulled away from the communities that need them most.Este borrado no es simbólico. Es operativo. Es el mecanismo mediante el cual se les arrebata el acceso, los servicios y la visibilidad a las comunidades que más los necesitan.
The public health system itself — the workforce that runs it, the data systems that inform it, and the institutions that give it credibility — is being dismantled through coordinated moves happening at the same time.17 The workforce is being purged at federal, state, and local levels.El propio sistema de salud pública — el personal que lo opera, los sistemas de datos que lo informan y las instituciones que le dan credibilidad — está siendo desmantelado mediante medidas coordinadas que ocurren al mismo tiempo.17 Se está purgando al personal a nivel federal, estatal y local.
"Civil servants are being fired left and right. They're being told from one day to the next that you no longer have a job because you said something or your job is considered DEI.""Están despidiendo a empleados públicos a diestra y siniestra. Les dicen de un día para otro que ya no tienen trabajo porque dijeron algo o porque su puesto se considera DEI."
National Nonprofit Leader (PT13)Líder de una organización sin fines de lucro de alcance nacional (PT13)
Data systems used to monitor and respond to the epidemic are being deliberately weakened.Los sistemas de datos que se usan para monitorear y responder a la epidemia están siendo debilitados de manera deliberada.
"This administration feels like they want to erase a lot of patient populations by not collecting data. This whole 2025 move seems like one not to track any HIV information. If you don't have the data, you can just pretend it doesn't exist.""Esta administración da la impresión de que quiere borrar a muchas poblaciones de pacientes simplemente al no recopilar datos. Toda esta movida de 2025 parece estar dirigida a no registrar ninguna información sobre el VIH. Si no tienes los datos, puedes hacer de cuenta que no existe."
Clinical Pharmacist (PT02)Farmacéutico clínico (PT02)
The credibility of public health institutions, and the information they produce, is actively undermined.La credibilidad de las instituciones de salud pública, y de la información que producen, está siendo socavada de manera activa.
"It is purposeful to intentionally remove the trust from what we knew as trusted scientific agencies — the CDC, the FDA, the ACIP.""Es a propósito: socavar intencionalmente la confianza en lo que conocíamos como agencias científicas de confianza — los CDC, la FDA, el ACIP."
National Nonprofit Leader (PT13)Líder de una organización sin fines de lucro de alcance nacional (PT13)
These are not three separate problems. Firing the people who collect the data, weakening the systems that house it, and undermining the institutions that publish it are lines of attack on the same target: the ability of public health to know what is happening, and to be believed when it says so.Estos no son tres problemas separados. Despedir a las personas que recopilan los datos, debilitar los sistemas que los albergan y socavar las instituciones que los publican son líneas de ataque contra un mismo blanco: la capacidad de la salud pública de saber qué está ocurriendo, y de que le crean cuando lo dice.